Are Covid vaccine mandates ethical? evidence based?
(This article was written in summer 2021. Since then, the evidence for many of the arguments made here has only become stronger, but I haven’t updated the article.)
Covid cases among the vaccinated are exploding even in some of the most vaccinated places on earth, e.g. Singapore, Israel, the UK, US. Although the infection rate among the vaccinated is still lower than the infection rate in unvaccinated, the difference has become rather small (certainly inconsistent with 95% efficacy) in many places. For example, in Singapore, at the time of writing this, 75% of the people were vaccinated and 66% of the recent cases were among vaccinated. Similarly, in the state of Massachusetts in the US, a week before writing this, ~70% of the people were fully vaccinated and 43% of the recent cases were among the vaccinated. The case numbers may be subject to sampling bias: for example, many places require only the unvaccinated to be tested, so we may be underestimating the number of vaccinated infected. One metric that is unaffected by such biases is death. More than half of the UK deaths were recently among the vaccinated at a time where 53% of the population was fully vaccinated. It is unclear what fraction of those deaths were in the fully vaccinated (vs partially vaccinated).
Instead of acknowledging the reduced effectiveness of vaccinations (due to variants and/or time since vaccination and/or …), governments are becoming even more and more mean towards the people who declined Covid vaccination or those who question the Covid vaccines. Many governments have started promoting the unvaccinated as second-class citizens worthy of only hatred and ostracization. Those asking even legitimate questions are brutally censored. Are the Covid unvaccinated to blame for the Covid infections of the vaccinated? This article analyses the common arguments.
If we knew for sure that Covid vaccines were perfectly safe, mandating them for everybody would be a no-brainer and this question wont ever arise. So, I first take a brief look at the safety concerns about the Covid vaccines and the ethics of mandating them.
Covid vaccine risk and ethics
Short-term risks
You can debate how low the adverse events rate of the Covid vaccines are, but they are non-trivial, both for mRNA vaccines and adenovirus-vector vaccines. (The Novavax vaccine, which uses a much more traditional (better understood and tested for decades) technology, may be much safer.) For example, despite that it is known that vaccine adverse event reporting systems underreport, the risk of usually-hospitalization-requiring myocarditis in young boys after mRNA vaccines is at least 1/20K. Similar is the overall risk of clots after the AstraZeneca vaccines. Already, many countries (unlike India) do not anymore recommend the AstraZeneca vaccine (also known as Covisheid, Vaxzevria) for the young because the risks outweigh benefits:
When Vaxzevria was used in younger age groups, the benefit–risk balance was no longer as favourable and even reversed in the younger age groups. For instance, using Vaxzevria in the entire adult population would avert four (95% PI: 2–7) COVID-19 deaths in the 18–29 year-olds and six (95% PI: 3–8) in the 30–39 year-olds, but it would be associated with 12 (95% PI: 7–19) and nine (95% PI: 6–14) deaths from TTS in these age groups, respectively.
Also important is to note that the vaccine adverse events, especially myocarditis, tend to be in people with much lower than average risk of dying from Covid. Thus, even though the known benefits of the vaccine may outweigh the known risks for an average person, it may not do so for every individual. Above, we already saw an example for AstraZeneca in young individuals. The risk benefit equation for the mRNA vaccines is also dicey for young boys, when comparing hospitalizations for Covid vs for myocarditis following Covid vaccines. In a more recent analysis, for boys 12-15 without medical comorbidities receiving their second mRNA vaccination dose, the rate of CAE (cardial adverse events, 86% of which required hospitalization) was 3.7 to 6.1 times higher than their 120-day COVID-19 hospitalization risk. This analysis was recently covered even in the Guardian, warranting caution.
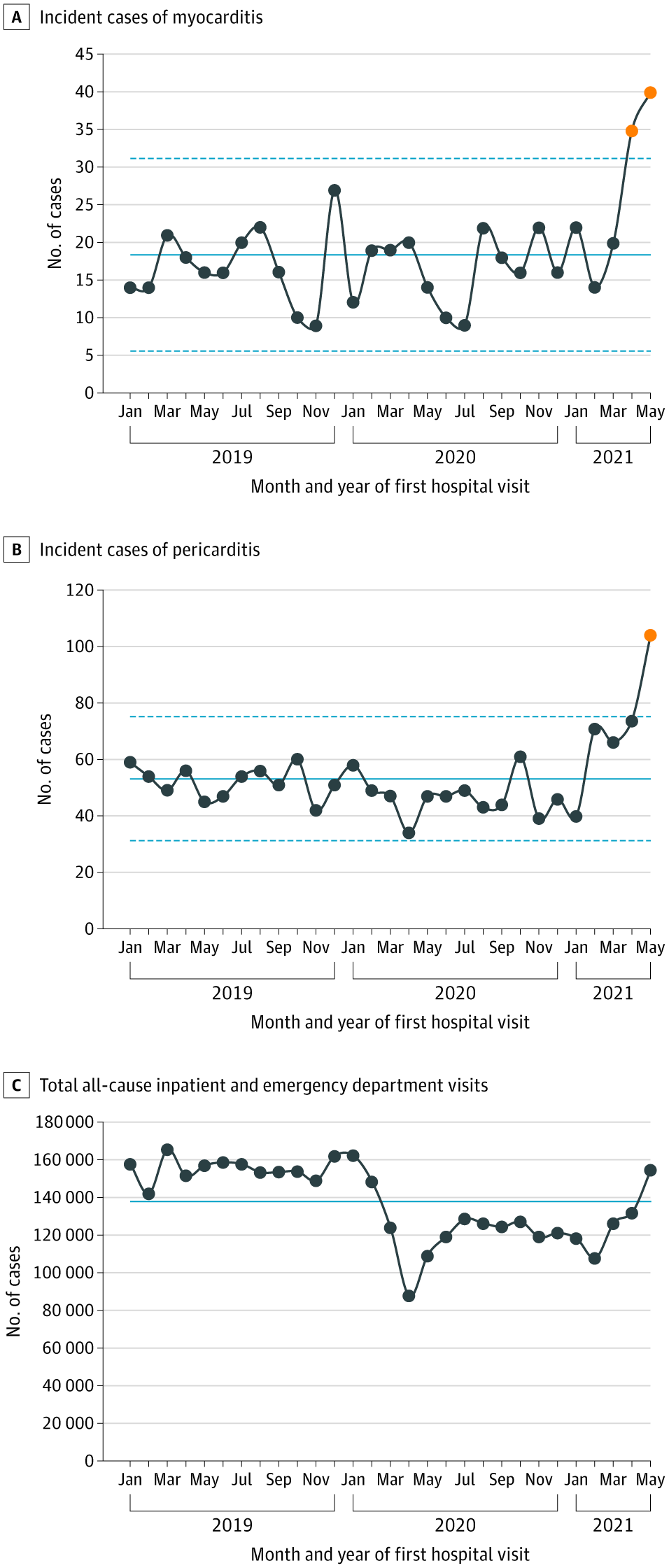
Some have claimed that Covid causes more myocarditis than Covid vaccines, but based on data that uses a much more permissive definition of myocarditis only when Covid is suspected to be the cause. Actually, the hospitalizations for myocarditis only rose after vaccinations started for the children, even though Covid had been around for a year by that time (the image is hyperlinked to the paper it was sourced from):
Also, many factors are known solidly to influence one’s risk from Covid upto even 10x, comparable to the risk reduction by Covid vaccines: e.g. Vitamin D deficiency, obesity and metabolic dysfunction, physical activity. (Just because no large trials were done to test inteventions like regular Vitamin D supplementation (or sun exposure), weight loss, physical exercise to prevent Covid infection/severity doesnt mean they are ineffective: until we test something properly, we cant say it doesnt work.) It is irresponsible to claim that the benefits outweigh risks for EVERYONE, perhaps just as irresponsible as extreme anti-vaxers confidently claiming that Covid vaccine risks outweigh benefits for everyone or will surely cause infertility.
Long-term risks
Clots and myocarditis are just the known short-term risks. There are several diseases like heart disease, cancer, that take decades to develop. Although there is no evidence that Covid vaccines cause them, no empirical evidence can exist that the Covid vaccines do NOT cause them. Given that lesions in coronary arteries (heart disease), which can eventually block arteries, at least progress via ASYMPTOMATIC (subclinical) clots, if not even initiate via clots, and that the adenovirus vaccines cause dangerous (symptomatic) clots in “rare” cases, and that the mRNA vaccines sometimes cause hospitalization-needing heart damage (inflammation) it is NOT implausible for these vaccines to cause heart problems (e.g. new lesions in arteries or worsening existing lesions) that are currently asymptomatic and show symptoms only after, say 5-10 years. Just because it is plausible doesnt mean it actually happens: fortunately, this plausibility can be disproven by an experiment: do a 2 year RCT of the Covid vaccines and do a non-invasive (but w/ radiation) CCTA test at the end of 2 years to look at the arteries in the heart: or measure a surrogate: the ultrasound CIMT test to evaluate lesions in the arteries supplying blood to brain.
Not only is there no long-term safety evidence, not much is being done to collect such evidence. Offering the vaccine to the placebo group essentially ended the RCT and thus will make it very difficult to reliably assess what the vaccine causes (both good/bad) in the long term. New drugs, e.g. in heart disease do normally require 2-3 year RCTs to rule out longer-term harms: and they are not even mandated by governments, which should require an even higher bar. Not even acknowledging the lower evidence bar for vaccines – which may be ethically justified – is not helping those who want to increase vaccine confidence. Just asserting long-term safety many times does not make it true, let alone believable by people who don’t think science is about blind belief in those with PhDs from American universities.
There may be theoretical evidence of the long-term safety of Covid vaccines. But theories in biology very often mispredict and there is a long history of introducing new interventions based on theoretical safety claims, whose harms were broadly recognized and acted upon decades later, often after prolonged smearing of those raising safety concerns:
- trans fats were banned after several decades of heavy promotion as a superior animal fat alternative
- after years after mass use starting as recently as 2015, the dengue vaccine was revealed to cause more severe disease among those who were not previously infected.
- the DDT inventor was given the nobel prize and was widely promoted even to kids. Only after several decades, after many questioning its safety, e.g. Rachel Carson, were smeared, it was banned. Many pesticides have a similar story: Endosulphan, suspected of causing birth defects in India, was only banned a decade ago.
- Merck’s Vioxx drug was withdrawn from the market after 5 years of public use and ads for causing an increased incidence of heart attacks
- after indiscriminate use of antibiotics for decades, it was found to cause not only antibiotic resistance but early overexposure is recently increasingly suspected to cause autoimmune diseases like asthma.
- Pthalates were introduced in 1920. We are still learning that they probably cause reproductive harm in humans.
- Clair Cameron Patterson suspected lead to be hamful as early as in 1940. But he was smeared for years before governments finally action on reducing lead exposure of the public only in 1970.
- the sugar for fat substitution promoted for decades is now increasingly believed to be harmful.
Coming back to Covid vaccines, exactly NONE of our expert theoreticians predicted the clots or myocarditis issues: in fact, they were very confidently claiming the opposite in December 2020. They don’t even understand the mechanisms of why these issues happen. Similarly, they dont know why the mRNA vaccines appear to cause menstural issues, or reactivation of some latent infections. (If they can reactivate latent viral infections, can the immune system changes caused by the vaccine even reactivate latent cancers, as as described by some reports in VAERS? Nobody knows. Covid-vaccines fanatics will correctly claim that we cannot generalize from these anecdotes and there is no reliable evidence Covid vaccines cause cancer. But cancer can take several years to develop and we ALSO not say for sure that Covid vaccines do NOT cause cancer until many years from now.) The existing mRNA vaccine theory didnt predict any of these (menstural issues, latent virus reactivation) either in December 2020. Ask any real scientist, e.g. Richard Feynman (perhaps the greatest physicist and science educator ever), and they will say theory that makes inaccurate predictions is WRONG, even if it is a beautiful theory of CDC/FDA/WHO:
Months after the wide promotion of the mRNA vaccines, we are still learning what happens to the mRNA vaccine contents in our bodies. When our understanding about them is so limited and has been proven to be wrong recently so many times (e.g. myocarditis), it is incorrect in my opinion to put too much faith in theoretical predictions from such limited understanding.
Ethics
Given such known > 1/20K short-term risks and largely unknown long-term risks of both the vaccines and the virus, I think Covid-vaccine mandates are deeply unethical: when there is a nontrivial risk and so many unknowns and so much variance in the risks from both the virus and the vaccines (the virus primarily harms the elderly but the vaccine’s KNOWN harms are concentrated in the young and healthy), Covid vaccination should be an individual choice: we all understand our bodies the best. However, for the rest of this article, I will forget about ethics and focus on the goal of reducing Covid transmission as much as possible, even if it comes at the cost of sacrificing a minority.
Do Covid vaccines reduce transmission? independent of symptoms?
To blame the unvaccinated for infections of the vaccinated, the first thing you have to establish is that the vaccines are highly effective in reducing the transmission of the virus.
However, none of the Covid randomized-controlled-trials (RCTs) were designed to measure that.
Many are assuming without proof that reducing symptomatic infections (which the RCTs showed) implies reduced transmission.
Assuming that reduction of symptoms implies reduced transmission is plausible.
But then why not discriminate based on symptoms rather than vaccination status?
Contact tracing data, although not fully reliable, does have many instances of transmision from vaccinated people to other people:
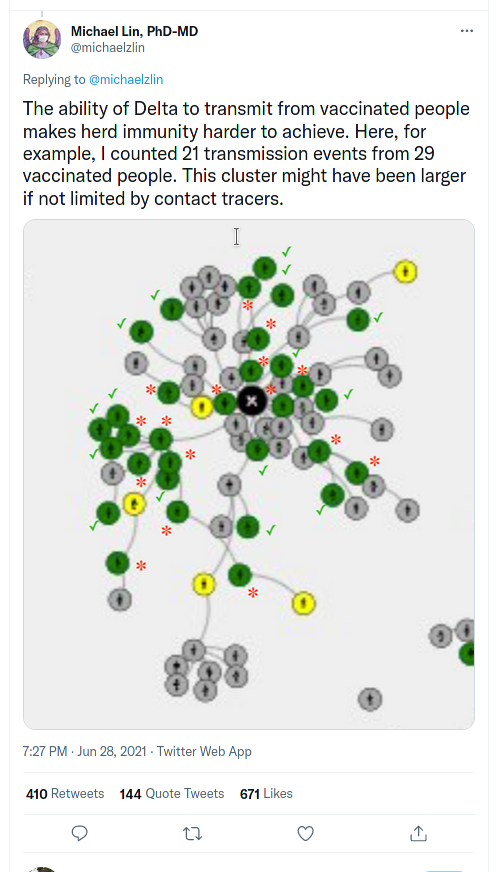
(twitter screenshots at this blog are hyperlinked to their source. In case the tweets get deleted, I certify that I took these screenshots myself on 25-July-2021.)
There is a recent anecdote of a vaccinated person with mild symptoms infecting “at least 60 people”. Also, a recent experiment found:
It is striking that relatively low Ct values (<20), i.e. high viral load, were found in 47% (16/34) of the employees who were fully vaccinated (Figure 1), without clear distinction in the type of vaccination (Figure 2).. All these 16 employees had complaints, with headache, fever and sore throat being the most frequently mentioned at the time of the test.
It is not yet known to what extent the virus secreted is infectious, but the combination of complaints with low Ct values makes contagiousness plausible. All these infections were contracted outside the hospital.
Fortunately, those cases of high viral load in vaccinated infected were all in those who had symptoms and not in asymptomatics. Although vaccines reduce symptomatic infections of the original variants at least for a few months, I have never seen any empirical evidence nor any plausible reason why a vaccinated infected person is less likely to transmit the virus than an unvaccinated infected person if they both have the same severity of symptoms. So perhaps a better strategy would be to request/require those with symptoms – even very minor ones – to isolate, including those who take symptom reduction interventions like Tylenol? It is surely not optimal if reducing Covid was the only goal of humanity and Covid was the only cause of human death, but is a good tradeoff in my opinion: it will stop the majority of the transmission and leave our societies mostly functional as before: life is about much more than being alive, and many people rightly believe that being locked down and away from human social contact and smiles for years is not a life worth living. Devising less invasive and more convenient at-home tests may also be a good approach during outbreaks: but this should not go on forever.
If the vaccinations reduce symptoms, which they likely do in the first few months after the second dose against the original variants, the vaccinated would be required less often to isolate, which is a fair perk for exposing oneself to the non-trivial known short-term adverse effects and the almost completely unknown long-term effects of the vaccines. Given that the mRNA vaccines are not completely safe and the later doses are riskier, requiring boosters every few months may be too risky to impose on everyone: even to kids whose risk of dying from Covid is ~10x less than the risk of suicide (see table 1 in this paper).
Covid-recovered are more immune to Covid variants than Covid vaccinated
A non-trivial fraction of the unvaccinated has already recovered from Covid, many didn’t even know they got Covid. For example, in New York city, this fraction was probably as high as 24.3% even in June-October 2020. The US Covid policy that is the hardest to explain by an ethics-free pursuit of Covid-circulation-minimization and can only be explained by insidious corruption of the governments and medical academia is the fact that at least in the US, even the Covid recovered are treated as second class citizens:
GMU’s unlawful policy mandates that all unvaccinated faculty, including those who can demonstrate natural immunity by way of prior Covid-19 infection, must wear a mask on campus, physically distance, and undergo frequent testing. Employees are also ineligible for merit-based pay increases if they do not upload proof of their vaccination status into an online portal. For Professor Zywicki, who has recovered from Covid-19 and acquired robust natural immunity, it is not only medically unnecessary to undergo a vaccination procedure at the current time, but doing so also would create a risk of harm to him. Nevertheless, because the penalties GMU attaches to remaining unvaccinated will diminish Professor Zywicki’s efficacy in performing his professional responsibilities, the policy coerces him into receiving the vaccine.
Some people claim that having a policy that has a lot of cases may be too complex for humans. I don’t think it is ethical to trade human lives (it is now well established that Covid vaccines have non-0 risk) for the complexity of having a policy with 2 cases. Furthermore, we can have a 1-case policy that only accepts an Covid antibody test results done anytime in the past. People who get infected or vaccinated should get an antibody test a few weeks after recovery or vaccination to show that they developed antibodies. It is true that antibody levels can wane after many months of Covid recovery, but that does not imply loss of immunity: at least the Covid recovered are known to produce memory immune cells (B cells) to remember the immune response for later. However, just after infection or vaccination (vs after many months), antibodies are supposed to detectable, if things are working as expected based on the current understanding of our immune system.
Even before variants, the available empirical evidence overwhelmingly suggested that the Covid-recovered are at as low risk (perhaps lower) of getting infected with Covid as the never infected Covid vaccinated. For example, in Israel:
Vaccination was highly effective with overall estimated efficacy for documented infection of 92·8% (CI:[92·6, 93·0]); hospitalization 94·2% (CI:[93·6, 94·7]); severe illness 94·4% (CI:[93·6, 95·0]); and death 93·7% (CI:[92·5, 94·7]). Similarly, the overall estimated level of protection from prior SARS-CoV-2 infection for documented infection is 94·8% (CI:[94·4, 95·1]); hospitalization 94·1% (CI:[91·9, 95·7]); and severe illness 96·4% (CI:[92·5, 98·3]). Our results question the need to vaccinate previously-infected individual
An analysis in the healthcare workers of the Cleveland Clinic Health System found the same
Of the 2154 SARS-CoV-2 infections during the study period, 2139 (99.3%) occurred among those not previously infected who remained unvaccinated or were waiting to get vaccinated, and15 (0.7%) occurred among those not previously infected who were vaccinated. Not one of the 2579 previously infected subjects had a SARS-CoV-2 infection, including 1359 who remained unvaccinated throughout the duration of the study
Most of India was battered during the recent second wave in April 2021. But one place that did not see a rise in infections or deaths is Dharavi, a very densely populated slum (917288 people per square mile) in India. Dharavi was battered by Covid in summer 2020 and had high prevalence of S-protein antibodies subsequently.
With Covid variants, reinfections may be more likely in both the vaccinated and the Covid recovered, but the variants appear to surpass the vaccine-derived immunity much much more easily than the immunity from previous infection(s):
With a total of 835,792 Israelis known to have recovered from the virus, the 72 instances of reinfection amount to 0.0086% of people who were already infected with COVID.
By contrast, Israelis who were vaccinated were 6.72 times more likely to get infected after the shot than after natural infection, with over 3,000 of the 5,193,499, or 0.0578%, of Israelis who were vaccinated getting infected in the latest wave.
This seems to hold not just for the delta variant, a CDC-published study of a gamma variant outbreak in a small group of gold miners showed:
The attack rate was 15/25 (60.0%) in fully vaccinated miners, 6/15 (40.0%) in those partially vaccinated or with a history of COVID-19, and 3/4 (75%) in those not vaccinated. Attack rate was 0/6 among persons with a previous history of COVID-19 versus 63.2% among those with no previous history (Table).
These observations are theoretically plausible: during natural infections, the body sees all of the virus and not just the spike protein, so what our bodies learn from natural infections is probably more robust to mutations in the spike protein. Researchers studying the robustness of natural immunity to Covid already found signs of it:
Recovered COVID-19 patients retain broad and effective longer-term immunity to the disease, suggests a recent Emory University study, which is the most comprehensive of its kind so far. The findings have implications for expanding understanding about human immune memory as well as future vaccine development for coronaviruses.
Ahmed says investigators were surprised to see that convalescent participants also displayed increased immunity against common human coronaviruses as well as SARS-CoV-1, a close relative of the current coronavirus. The study suggests that patients who survived COVID-19 are likely to also possess protective immunity even against some SARS-CoV-2 variants.
“Vaccines that target other parts of the virus rather than just the spike protein may be more helpful in containing infection as SARS-CoV-2 variants overtake the prevailing strains,” says Ahmed. “This could pave the way for us to design vaccines that address multiple coronaviruses.”
More abstractly, immune systems across species have evolved for billions of years to fight natural infections that replicate inside our bodies, and they may not be as well adapted to the mechanisms of PEG/mRNA or non-replicating adenoviruses. For many other disease, e.g. measles, natural immunity is known to be much more robust than immunity provided by the very effective and safe MMR vaccine.
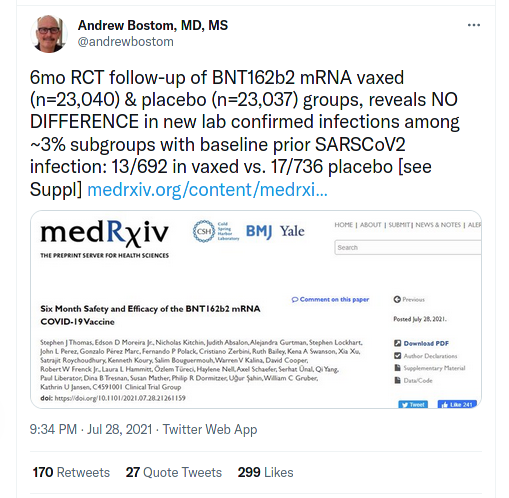
Even though the vaccine appears to provide much weaker immunity than a natural Covid infection, especially w.r.t variants, does the Covid vaccine provide additional protection to those who were already infected? There is some recent observational data showing that vaccination reduces the already very small chances of reinfection, although that may not be true of the latest variants. Also, because there are many known confounders: e.g. many situations, e.g. travel, only require the unvaccinated to be tested. In fact, a few months ago, the CDC decided not to track mild or asymptomatic Covid infections, but only in the vaccinated. RCTs can separate correlation/biases from causation and a Covid vaccine RCT should be done on the previously recovered before subjecting them to unnecessary harm. Meanwhile, the Pfizer Covid vaccine RCT already sheds some light on this, although the number of reinfections were very small in both the vaccinated and the unvaccinated groups:
Also, note that those with previous Covid recovery appear to have a higher rate of adverse effects from the vaccines:
The proportion reporting one moderate/severe symptom was higher in the previous COVID-19 group (56% v 47%, OR=1.5 [95%CI, 1.1–2.0], p=.009), with fever, fatigue, myalgia-arthralgia and lymphadenopathy significantly more common.
In the coming months, today’s unvaccinated never Covid infected will either be dead or Covid recovered
Given how infectious some of the new variants are, it is likely that many of those who are unvaccinated and never had Covid will get it within a few months if not a year. They may die in which case most people will be happy, given the tremendous amount of hate the governments have promoted against the unvaccinated. If they recover, they will likely have more robust immunity against the variants than the vaccinated, thus contributing MORE to controlling the pandemic than the vaccinated never infected.
One concern is that they may spread the virus while recovering or dying. A policy that asks the symptomatics (vaccinated or not) to isolate will prevent most of such transmissions. It may miss some, but as discussed above, there is no empirical evidence (that I know of) that vaccinated asymptomatically infected are less likely to transmit a virus than the unvaccinated asymptomatically infected, so it is unjust to discriminate between the two groups. It may also be fair to deprioritize Covid-related hospital/ICU admissions of the unvaccinated in case the hospital systems are overloaded.
To summarize, instead of treating the currently unvaccinated never infected as the cancer of our societies, look at the positive side: in the coming months, most of them will either die from Covid and cease to be a problem for others or recover from Covid and contribute MORE to controlling the pandemic than the vaccinated never infected.
Leaky Covid vaccines and evolutionary pressure
Many have alleged that the unvaccinated are mutant factories.
The claim was that because vaccines prevent infection, they prevent transmission,
thus they give the virus much less chance to evolve, as summarized by one of the most trusted
vaccine advocates of worldwide media:
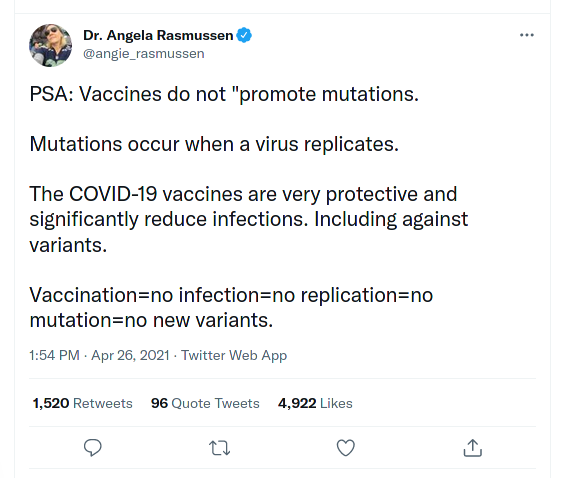
“Vaccination=no infection” may have been a reasonable thing to say at that time when vaccines were about 95% effective in reducing symptomatic infections. Even then, it was not clear whether they reduce infections overall (including asymptomatic ones) as much as 95%. Now, such a claim is very very wrong. As mentioned above, in Singapore, at the time of writing this, 75% of the people were vaccinated and 66% of the recent cases were among vaccinated. (It is not just because of the new variants: there is at least one genome-sequencing confirmed case of alpha-variant transmission from a vaccinated person with no immune deficiency.) It has been known that such leaky vaccines that do not prevent infections promote mutations that can be more virulent and more deadly:
Here we show that vaccines designed to reduce pathogen growth rate and/or toxicity diminish selection against virulent pathogens. The subsequent evolution leads to higher levels of intrinsic virulence and hence to more severe disease in unvaccinated individuals. This evolution can erode any population-wide benefits such that overall mortality rates are unaffected, or even increase, with the level of vaccination coverage. In contrast, infection-blocking vaccines induce no such effects, and can even select for lower virulence. These findings have policy implications for the development and use of vaccines that are not expected to provide full immunity, such as candidate vaccines for malaria.
The Covid vaccines were never perfect at infection blocking and never provided full immunity. Now, the infection-blocking capacity of Covid vaccines seems much much lower. The vaccines may still be effective in reducing severe disease in the vaccinated. The variants that thrive the most in the vaccinated hosts would be those who transmit better among the vaccinated and yet are not too deadly to their vaccinated hosts (killing hosts can reduce spread), but there little selection pressure against variants that are very deadly to the unvaccinated, especially if the majority of the population is vaccinated. So this may lead to variants that are more virulent among the vaccinated and more deadly in the unvaccinated. This phenomena was observed even in the case of human vaccines:
A new vaccine called Prevnar 7 was soon to be recommended for all U.S. children to prevent infections caused by Streptococcus pneumoniae, bacteria responsible for many cases of pneumonia, ear infections, meningitis and other illnesses among the elderly and young children.
while Prevnar 7 almost completely eliminated infections with the seven targeted serotypes, the other, rarer serotypes quickly swept in to take their place, including a serotype called 19A, which began causing a large proportion of serious pneumococcal infections. In response, in 2010, the U.S. introduced a new vaccine, Prevnar 13
Overall, the incidence of invasive pneumococcal infections in the U.S. has dropped dramatically among children and adults as a result of Prevnar 13 (vaccine). It is saving many American lives, presumably because it targets the subset of serotypes most likely to cause infections. But data from England and Wales are not so rosy. Although infections in kids there have dropped, invasive pneumococcal infections have been steadily increasing in older adults and are much higher now than they were before Prevnar 7 was introduced. As for why this is happening, “I don’t think we know,” Hanage said. “But I do think that we might somewhat reasonably suggest that the serotypes that are now being carried by children are inadvertently better able to cause disease in adults, which is something we would not have known before, because they were comparatively rare.”
Although the delta variant may have originated before Covid vaccines were available to the public, it may have originated after the onset of the vaccine trials all over the world. In either case, mass vaccination may have caused it to thrive much better because of its better virulence (vs the original variant) among the vaccinated.
There actually are Covid vaccines that do appear to provide complete blocking of transmission (also known as sterlizing immunity), but they use a centuries old technology (live-attenuated viruses) known to have eradicated many diseases, not the novel mrna technology with extra-ordinary hype but dismal safety and efficacy. Most of this article does not apply to that live-attenuated vaccine, but I doubt it will receive attention and be brought to the market as a much better alternative to the current Covid vaccines.
Conclusion
It is true that people at risk of severe disease should strongly consider getting vaccinated for their own benefit. But if they chose to not get vaccinated, the currently known evidence does not support the claim that they are putting the vaccinated people at risk of Covid by not getting vaccinated. It may be fair to deprioritize the Covid treatment of the unvaccinated, especially in case of hospital overflows. But governments, media, and the “experts” should refrain from sowing hatred against the unvaccinated and refrain from discriminating based on vaccination status, not just because it is unethical given the non-trivial risks of the vaccines, but also because it is not supported by evidence as far as I know.
You can contribute to this post by making a merge request to this file.